
 Presidential fatigue has been much in the news of late. And has been, since the dawning days of the Obama presidency (recall the excuses for the DVD set gifted to the British?). Why is anyone surprised? This is, as far as I can tell, Obama's longest running gig since college. Unless Obama pulls a Palin, he's locked into the longest obligation he's ever had to navigate.
Presidential fatigue has been much in the news of late. And has been, since the dawning days of the Obama presidency (recall the excuses for the DVD set gifted to the British?). Why is anyone surprised? This is, as far as I can tell, Obama's longest running gig since college. Unless Obama pulls a Palin, he's locked into the longest obligation he's ever had to navigate.
Thursday, December 31, 2009
Obama's Longest Gig
Presidential fatigue has been much in the news of late. And has been, since the dawning days of the Obama presidency (recall the excuses for the DVD set gifted to the British?). Why is anyone surprised? This is, as far as I can tell, Obama's longest running gig since college. Unless Obama pulls a Palin, he's locked into the longest obligation he's ever had to navigate.
Friday, November 20, 2009
Senator Sherrod Brown's Fatally Flawed Logic about Health Care Reform
I recently emailed Senator Sherrod Brown to urge him to vote no on the "health care" legislation currently before the Senate. In response, Senator Brown's office sent the reply reproduced below. The Senator and I agree that there is room for reform in the health sector. The Senator's rationale for supporting the current "health care" legislation before the Senate is fatally flawed. The Senator appears unfamiliar with the factors that drive health care costs. Were he familiar with those factors, he would realize that the solution he advocates intensifies the inefficiencies inherent in the existing health. Only measures that (1) shift system focus to outcomes and managing disease states, rather than delivering services, and (2) stimulate and reward innovation will bring about improved health outcomes AND lower costs.
I recommend the Senator read Michael Porter's book Redefining Health Care as a start.
The Senator's illogic follows:
I recommend the Senator read Michael Porter's book Redefining Health Care as a start.
The Senator's illogic follows:
Sherrod Brown
to me
Dear Dr. Kleine:
Thank you for sharing your views on health reform.
With health care costs rising to a breaking point and access to health coverage rapidly eroding, our health care system is in need of reform. We must reduce the long-term growth of health care costs for patients, taxpayers, and businesses; protect families from bankruptcy or debt because of health expenditures; guarantee a choice of doctors and health plans; invest in prevention and wellness; improve patient safety and quality of care; assure affordable, quality health coverage for all Americans; and end barriers to coverage for people with pre-existing conditions.
One promising solution to the problems of cost, quality, and access that plague our health care system is to increase competition in the health insurance market. If the private insurance industry was truly competitive, then there would be strong incentives to provide coverage to as many Americans as possible and to build customer loyalty through cost savings and quality improvements. Unfortunately, insurers do not truly compete against one another; instead, they make use of the same basic strategies to earn significant profits. These tactics include selectively insuring the lowest risk enrollees, slow-walking claims payments so they can earn interest on every premium dollar, and denying as many claims as possible.
What the insurance industry needs is some healthy competition from a public insurance option. This option would not replace employer-sponsored coverage and no one would be forced into it; the public option would simply give uninsured or underinsured Americans the choice of enrolling in a quality, affordable health insurance plan that does not engage in the same cost-avoidance tactics that some private insurance plans do. The public health insurance option would also be a vehicle for improvements in quality, coverage, and provider-access that sets the bar higher for private insurance plans. This option would be available to all Americans: both private and government employees, including members of Congress and their staffs.
Since Congress began debating health reform, an overwhelming number of people in Ohio have contacted me. I appreciate this input and am carefully considering the thoughts, questions, and concerns that you and other Ohioans have shared with me.
One question I am often asked is whether I would enroll in the public insurance option. Since first coming to Congress in 1993, I have refused to enroll in the coverage offered to members of Congress until every American has access to high-quality, affordable health insurance. Should a health care reform bill pass that offers a public insurance option, I would be pleased to enroll.
I have also heard from Ohioans concerned about proposals to tax employer-sponsored benefits. I am opposed to taxing these benefits, which would unjustifiably increase the cost of health insurance for working families in Ohio.
Several Ohioans have also questioned whether Americans should be required to purchase coverage. They have expressed concerns over establishing fines intended to increase participation in the health insurance system.
It is important to clarify that these fines would not affect anyone who is currently insured. One of the key principles of the reform effort is that Americans who are satisfied with their coverage today should be able to keep it without being subject to additional costs. However, without a mechanism that encourages the purchase of insurance, some individuals will continue to forego coverage, resulting in uncompensated care costs that inflate insurance premiums and increase the costs of Medicare and Medicaid.
Unfortunately, too many Americans today forego health insurance not by choice, but by circumstance. Many Americans are left without health insurance because their employers don’t offer it, and because it is too expensive to buy in the individual market. That’s why I am working to ensure that individuals who cannot afford the high costs of coverage are provided with federal subsidies to help them purchase insurance. I recognize that, even with federal help, some individuals will still not be able to afford health insurance and I firmly believe that those individuals should not have to pay any fines because they are unable to afford health insurance.
A consolidated Senate health reform bill, the “Patient Protection and Affordable Care Act,” was released on November 18, 2009, and will be considered by the Senate over the next few weeks. According to the Congressional Budget Office (CBO), this bill would extend coverage to an additional 31 million Americans, would cost approximately $848 billion to implement, and would reduce the national deficit by $130 billion over the next decade. The bill is available online athttp://democrats.senate.gov/reform/patient-protection- affordable-care-act.pdf.
On November 7, 2009, the House of Representatives passed legislation, the Affordable Health Care for America Act (H.R. 3962), by a vote of 220 to 215. For more information on the House of Representatives’ health reform bill, please visit http://www.speaker.gov/newsroom/legislation?id=0327.
I am currently reviewing the Senate bill, but am pleased we are one step closer to passing health reform legislation beneficial to health care consumers, businesses, and taxpayers alike. I also support giving every member of Congress, and every member of the public, time to review the bill.
As Congress moves forward on health reform, I will certainly work to address the issues contained in your letter. If you wish to learn more about my work on health reform as well as the most Frequently Asked Questions (FAQs) that Ohioans have posed to my office, please visit my website at:
http://brown.senate.gov/issues_and_agenda/stories/ share/?issue_id=f565635b-e37a- 45d3-b15f-edf6b930bd1a.
Thank you again for getting in touch with me on this important matter.
Sincerely,
Sherrod Brown
United States Senator
Wednesday, November 18, 2009
Recovery.gov: The New Transparency
Much has been made this week of the Recovery.gov database (here and here, for example). Some are of the opinion that listing TARP dollars spent in nonexistent congressional districts -- such as the $752,292 spent in Texas Congressional District #00 -- are errors.
I believe these reports are part of the new Obama regime transparency standards. It seems plausible that Obama is being completely transparent about where TARP funds are going. It seems reasonable that the codes that don't map to known congressional districts, instead designate uses of the funds for purposes that don't benefit the congressional districts (e.g., graft, political war chests, ACORN, etc.). Yep, complete transarency!
The lingering question is: who will decipher those non-valid district codes?
Update: Congress to investigate phantom Congressional districts. THAT ought to be entertaining. If the districts are fake, is the investigation real?
Update 2: Bosse for NHCD 00. Oh, the fun factor is following a hockey-stick trajectory.
I believe these reports are part of the new Obama regime transparency standards. It seems plausible that Obama is being completely transparent about where TARP funds are going. It seems reasonable that the codes that don't map to known congressional districts, instead designate uses of the funds for purposes that don't benefit the congressional districts (e.g., graft, political war chests, ACORN, etc.). Yep, complete transarency!
The lingering question is: who will decipher those non-valid district codes?
Update: Congress to investigate phantom Congressional districts. THAT ought to be entertaining. If the districts are fake, is the investigation real?
Update 2: Bosse for NHCD 00. Oh, the fun factor is following a hockey-stick trajectory.
Monday, October 05, 2009
Consumers Union Goes All Political ... Time to Cancel my Subscription?
Below is the content of an email I just sent to Consumers Union:
Consumer Report's position on the health sector has the appearance of political posturing and lacks Consumer Report's neutral perspective. It appears that Consumer's Union is violating its mission in how it has chosen to address the health sector (for example: http://legalinsurrection.blogspot.com/2009/10/consumer-reports-specious-stand-on.html
and also
http://theblogprof.blogspot.com/2009/10/supposedly-neutral-consumer-reports.html
As a long-time subscriber to Consumer Reports these violations of Consumer Union's mission has me on the verge of cancelling my print and online subscriptions as Consumers Union has afforded me reason to question the veracity of its reporting.
Clayton Christensen and Michael Porter recently released books that critique the US Health Sector. Interestingly, neither book affords support to the models advocated by CU.
What is Consumers Union's response to mission violations? Does Consumers Union intend to continue following its current path on the health sector which undermines CU's credibility in my eyes? Has CU chosen to alter its mission and become a political advocate? Why should I continue to trust CU's evaluations of products generally, and assessment of the health sector specifically?It will be interesting to see whether they reply.
Monday, August 31, 2009
What Happened to Live Free or Die?
New Hampshire congresswoman Carol Shea-Porter has police eject a constituent because he lacked a 'golden ticket'. What happened to New Hampshire's Live Free or Die attitude?
Monday, August 24, 2009

Thursday, August 20, 2009
Short Life
One has to wonder: Would Obama's health plan would have a life-span akin to the duration of the cash for clunkers program?
I Support the Law ... Except when it's inconvenient
The ailing Senator Ted Kennedy:
“I strongly support that law and the principle that the people should elect their senator,’’ Kennedy wrote. “I also believe it is vital for this Commonwealth to have two voices speaking for the needs of its citizens and two votes in the Senate during the approximately five months between a vacancy and an election.’’So, the Senator is law abiding except when the law is inconvenient to his priorities. Given the Senator's obvious familiarity with Massachusetts's Senate succession law, and its implications, he should have planned his resignation from the senate accordingly.
Wednesday, August 19, 2009
Guiding Principles Health for Care Innovation: Some Initial Thoughts
As discussion about the health care sector approaches a full howl, here are some thoughts regarding principles I believe should be guiding discussion about health care innovation:
1. Change the reward structure. A major problem with the health care system is that it rewards treating the sick. I believe the system should be re-imagined as a wellness support system. By increasing the baseline wellness level, resources needed to treat illness due to preventable causes, overall cost of health expenditures would reduce freeing up resources that could be directed elsewhere (perhaps to aid those with catastrophic health issues such as your friend). This tool lets you fiddle with wellness ROI. Essential to wellness program success is careful targeting of behaviors to change.
2. Personal responsibility. I believe that health is a personal responsibility. We each have a responsibility to actively pursue a health. System incentives should be aligned with pursuit of healthful life.
Incentives in the form of modest co-pays, and the like, insulate consumers from the cost of health care. Consumers, rationally, are less price sensitive as a result. Consumers need to have incentive to be concerned about the cost of health services. Increasing price sensitivity of consumers will increase pricing pressure on health care providers.
3. Empower innovation. Innovation is the only path to reducing the cost of health services while simultaneously increasing the quality of health care. Encourage entrepreneurs to do what they do so well: create effective solutions to problems. Innovation is needed in myriad areas, including diagnostic and delivery technologies and in business models. Christensen, in The Innovator's Prescription: A Disruptive Solution for Health Care , provides an outstanding blueprint for how to empower innovation in the health care sector.
, provides an outstanding blueprint for how to empower innovation in the health care sector.
A challenge of innovation is that innovation spurs changes in consumer expectations. Expectations re. what the health care system can deliver (e.g., ., what can be treated) are a function of the system's ability to innovate and get rewarded for that innovation. The more the system can deliver, the more we expect of the system; the more treatment we expect to be included in our health care coverage.
4. Focus on outcomes rather than inputs or specific solutions. A focus on outcomes spurs innovation that can yield better outcomes at lower costs. A focus on outcomes is consumer-centric; it puts the focus on quality of patient care rather than on the caregiver.
5. Health care, is a complex adaptive system. System improvement is a function of the system being able to cycle, adapt, and 'emerge'. This implies identifying and removing barriers that inhibit system innovation and adaptation.
6. The market is smarter than any individual entity (human or organization). Ergo, the health care system will operate most efficiently -- yielding the optimal patient outcomes -- when barriers to market function are systematically identified and removed.
These thoughts are necessarily incomplete and preliminary.
1. Change the reward structure. A major problem with the health care system is that it rewards treating the sick. I believe the system should be re-imagined as a wellness support system. By increasing the baseline wellness level, resources needed to treat illness due to preventable causes, overall cost of health expenditures would reduce freeing up resources that could be directed elsewhere (perhaps to aid those with catastrophic health issues such as your friend). This tool lets you fiddle with wellness ROI. Essential to wellness program success is careful targeting of behaviors to change.
2. Personal responsibility. I believe that health is a personal responsibility. We each have a responsibility to actively pursue a health. System incentives should be aligned with pursuit of healthful life.
Incentives in the form of modest co-pays, and the like, insulate consumers from the cost of health care. Consumers, rationally, are less price sensitive as a result. Consumers need to have incentive to be concerned about the cost of health services. Increasing price sensitivity of consumers will increase pricing pressure on health care providers.
3. Empower innovation. Innovation is the only path to reducing the cost of health services while simultaneously increasing the quality of health care. Encourage entrepreneurs to do what they do so well: create effective solutions to problems. Innovation is needed in myriad areas, including diagnostic and delivery technologies and in business models. Christensen, in The Innovator's Prescription: A Disruptive Solution for Health Care
A challenge of innovation is that innovation spurs changes in consumer expectations. Expectations re. what the health care system can deliver (e.g., ., what can be treated) are a function of the system's ability to innovate and get rewarded for that innovation. The more the system can deliver, the more we expect of the system; the more treatment we expect to be included in our health care coverage.
4. Focus on outcomes rather than inputs or specific solutions. A focus on outcomes spurs innovation that can yield better outcomes at lower costs. A focus on outcomes is consumer-centric; it puts the focus on quality of patient care rather than on the caregiver.
5. Health care, is a complex adaptive system. System improvement is a function of the system being able to cycle, adapt, and 'emerge'. This implies identifying and removing barriers that inhibit system innovation and adaptation.
6. The market is smarter than any individual entity (human or organization). Ergo, the health care system will operate most efficiently -- yielding the optimal patient outcomes -- when barriers to market function are systematically identified and removed.
These thoughts are necessarily incomplete and preliminary.

Cash for Clunker (in)Competence

Hundreds of auto dealers in the New York area have withdrawn from the government's Cash for Clunkers program, citing delays in getting reimbursed by the government, a dealership group said Wednesday.
The Greater New York Automobile Dealers Association, which represents dealerships in the New York metro area, said about half its 425 members have left the program because they cannot afford to offer more rebates. They're also worried about getting repaid.And Obama expects us to believe claims that expanding government involvement in the health sector will improve quality of care and reduce costs?
Sunday, August 16, 2009
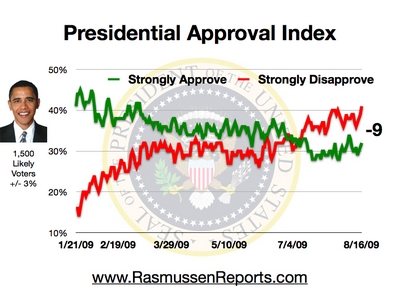
Obama's Negatives Continue to Build
Obama scores a -9 in Rasumssen's latest Presidential approval tracking poll:

That the strongly disapproves and strongly approves both ticked up in this latest poll may suggest that the middle is tipping toward strongly disapprove. The data also suggest public opinion is trending against Obama.. This tweaking of Rasmussen's graph emphasizes Obama's reversal of fortune:

That the strongly disapproves and strongly approves both ticked up in this latest poll may suggest that the middle is tipping toward strongly disapprove. The data also suggest public opinion is trending against Obama.. This tweaking of Rasmussen's graph emphasizes Obama's reversal of fortune:

Apple is Enablng 2009 to be 1984
Apple's famous '1984' ad concluded, "On January 24th, Apple Computer will introduce MacIntosh. You'll see why 1984 won't be like "1984":
Scott Ott illustrates how Apple is enabling 2009 to be like "1984". Yep, there's an app for that:
Scott Ott illustrates how Apple is enabling 2009 to be like "1984". Yep, there's an app for that:
The Health Care Diversion: It's the Economy, Stupid

One has to wonder: Is the Democrat's emphasis on health care a diversionary tactic? Sure, there is room for improvement in the U.S. health care system. Is a whole-sale make-over of the U.S. health care system needed? I don't read the tea leaves that way.
The momentum for whole-sale reform of the U.S.'s health care system is premised on a sour U.S. and world economy. The logic may go thus: The more people there are out of work, the more people there are that may be interested in government health care. Hence, the Obama administration has incentive to delay the recovery of the U.S. economy to increase the likelihood of passing government-run health care. My intent here is not to be conspiratorial. However, Rahm Emmanual's infamous, "Don't waste a 'serious crisis" comment, affords a basis for skepticism. The depressed U.S. economy affords just such a 'crisis' that can be 'leveraged.'
Issues with the U.S. health care system are meaningfully a function of the state of the U.S. economy. The healthier the U.S. economy, the more wealth there is available in the private sector. Wealth in the private sector reflects job creation, salary and benefits expansion, increased charitable giving to non-profit hospitals and other community support organizations, and greater freedom of individual choice. These, collectively, reduce the need for government involvement in health care.
The current government efforts to reconfigure the U.S. health care system reflect an attempt to address perceived systemic symptoms without an initial diagnosis. Proposed measures are akin to treating a fever generated by a bacterial infection with an ice-pack. The ice-pack is noticeable, and appears to offer relief, yet has no therapeutic impact on the underlying infection.
The considerable effort pouring into health sector reconfiguration focuses on a symptom that diverts energy and attention away from the underlying weakness of the U.S. economy. The focus on health sector reform is a diversion that pulls energy and focus away from engaging discussion on what is needed to ensure the long-term health of the U.S. economy; to engage entrepreneurial efforts that create jobs; to divert attention away from the fact that the U.S. economy continues to shed jobs.
To reprise a phrase popular with the last Democrat to occupy the White House: It's the economy, stupid. Getting the U.S. economy back on solid footing would seem to go a long way to improving the health care experience of every U.S. citizen and do so in a way that generates, rather than consumes, wealth and health for all.
The IRS and Your Health Care

Under both the House and Senate Health, Education, Labor and Pensions (HELP) Committee bills released to the public, the Internal Revenue Service will play a key role in monitoring and enforcing health care mandates against individual taxpayers. Yet the introduction of the IRS into the health care system has received scant attention.
The Senate bill imposes a new requirement that all persons who provide health care coverage to others must file a return with the IRS listing the names, addresses, social security numbers, and the coverage period for each person, and "such other information as the Secretary [of Health and Human Services] may prescribe." (Section 161(b) starting at page 107). The bill does not limit what information the Secretary may request, so it is conceivable and likely that information as to the nature of the coverage, the family members included, and other details will be reported to the IRS.
Read the whole thing. Would you want the IRS to be monitoring your health care and have the power to decide whether you have paid properly for care received?
Tuesday, May 26, 2009

Saturday, May 23, 2009
President Oblivious
Drudge is featuring this stunning interview excerpt of C-SPAN host Steve Scull with President Obama:
Stunning. Simply stunning. President oblivious.
UPDATE: Glenn Reynolds puts it succinctly:

SCULLY: You know the numbers, $1.7 trillion debt, a national deficit of $11 trillion. At what point do we run out of money?Is Obama suggesting that the current deficits -- deficits created by legislation signed by Obama since he became President -- don't count because they are "not caused by any decisions we've made on healthcare so far."? What does healthcare have to do with the current deficits? Does Obama not realize that his ideas for the healthcare system will further the increase in federal spending on healthcare, further increasing federal obligations and deficits? Is Obama oblivious to the billions of dollars that have been spent on projects -- like forced lending to financial institutions and purchasing auto companies -- and earmark sweetheart deals for congressional and senate districts are responsible for the current tsunami of federal spending? Is Obama oblivious to how his administrations intervention with the capital markets has poisoned the atmosphere for investment?
OBAMA: Well, we are out of money now. We are operating in deep deficits, not caused by any decisions we've made on health care so far. This is a consequence of the crisis that we've seen and in fact our failure to make some good decisions on health care over the last several decades.
So we've got a short-term problem, which is we had to spend a lot of money to salvage our financial system, we had to deal with the auto companies, a huge recession which drains tax revenue at the same time it's putting more pressure on governments to provide unemployment insurance or make sure that food stamps are available for people who have been laid off.
So we have a short-term problem and we also have a long-term problem. The short-term problem is dwarfed by the long-term problem. And the long-term problem is Medicaid and Medicare. If we don't reduce long-term health care inflation substantially, we can't get control of the deficit.
So, one option is just to do nothing. We say, well, it's too expensive for us to make some short-term investments in health care. We can't afford it. We've got this big deficit. Let's just keep the health care system that we've got now.
Along that trajectory, we will see health care cost as an overall share of our federal spending grow and grow and grow and grow until essentially it consumes everything...
Stunning. Simply stunning. President oblivious.
UPDATE: Glenn Reynolds puts it succinctly:
So we’re out of money because we don’t have national health care? Bogus. I think, instead, that it has something to do with the fact that Obama has been pouring money down a crony-statist rathole at absolutely astronomical and unprecedented rates. Yep, here’s that graphic again. Note that it doesn’t support Obama’s claim at all — but it does support mine.

Subscribe to:
Posts (Atom)