
New Hampshire congresswoman Carol Shea-Porter has police eject a constituent because he lacked a 'golden ticket'. What happened to New Hampshire's Live Free or Die attitude?
Monday, August 31, 2009
Monday, August 24, 2009

Thursday, August 20, 2009
Short Life
One has to wonder: Would Obama's health plan would have a life-span akin to the duration of the cash for clunkers program?
I Support the Law ... Except when it's inconvenient
The ailing Senator Ted Kennedy:
“I strongly support that law and the principle that the people should elect their senator,’’ Kennedy wrote. “I also believe it is vital for this Commonwealth to have two voices speaking for the needs of its citizens and two votes in the Senate during the approximately five months between a vacancy and an election.’’So, the Senator is law abiding except when the law is inconvenient to his priorities. Given the Senator's obvious familiarity with Massachusetts's Senate succession law, and its implications, he should have planned his resignation from the senate accordingly.
Wednesday, August 19, 2009
Guiding Principles Health for Care Innovation: Some Initial Thoughts
As discussion about the health care sector approaches a full howl, here are some thoughts regarding principles I believe should be guiding discussion about health care innovation:
1. Change the reward structure. A major problem with the health care system is that it rewards treating the sick. I believe the system should be re-imagined as a wellness support system. By increasing the baseline wellness level, resources needed to treat illness due to preventable causes, overall cost of health expenditures would reduce freeing up resources that could be directed elsewhere (perhaps to aid those with catastrophic health issues such as your friend). This tool lets you fiddle with wellness ROI. Essential to wellness program success is careful targeting of behaviors to change.
2. Personal responsibility. I believe that health is a personal responsibility. We each have a responsibility to actively pursue a health. System incentives should be aligned with pursuit of healthful life.
Incentives in the form of modest co-pays, and the like, insulate consumers from the cost of health care. Consumers, rationally, are less price sensitive as a result. Consumers need to have incentive to be concerned about the cost of health services. Increasing price sensitivity of consumers will increase pricing pressure on health care providers.
3. Empower innovation. Innovation is the only path to reducing the cost of health services while simultaneously increasing the quality of health care. Encourage entrepreneurs to do what they do so well: create effective solutions to problems. Innovation is needed in myriad areas, including diagnostic and delivery technologies and in business models. Christensen, in The Innovator's Prescription: A Disruptive Solution for Health Care , provides an outstanding blueprint for how to empower innovation in the health care sector.
, provides an outstanding blueprint for how to empower innovation in the health care sector.
A challenge of innovation is that innovation spurs changes in consumer expectations. Expectations re. what the health care system can deliver (e.g., ., what can be treated) are a function of the system's ability to innovate and get rewarded for that innovation. The more the system can deliver, the more we expect of the system; the more treatment we expect to be included in our health care coverage.
4. Focus on outcomes rather than inputs or specific solutions. A focus on outcomes spurs innovation that can yield better outcomes at lower costs. A focus on outcomes is consumer-centric; it puts the focus on quality of patient care rather than on the caregiver.
5. Health care, is a complex adaptive system. System improvement is a function of the system being able to cycle, adapt, and 'emerge'. This implies identifying and removing barriers that inhibit system innovation and adaptation.
6. The market is smarter than any individual entity (human or organization). Ergo, the health care system will operate most efficiently -- yielding the optimal patient outcomes -- when barriers to market function are systematically identified and removed.
These thoughts are necessarily incomplete and preliminary.
1. Change the reward structure. A major problem with the health care system is that it rewards treating the sick. I believe the system should be re-imagined as a wellness support system. By increasing the baseline wellness level, resources needed to treat illness due to preventable causes, overall cost of health expenditures would reduce freeing up resources that could be directed elsewhere (perhaps to aid those with catastrophic health issues such as your friend). This tool lets you fiddle with wellness ROI. Essential to wellness program success is careful targeting of behaviors to change.
2. Personal responsibility. I believe that health is a personal responsibility. We each have a responsibility to actively pursue a health. System incentives should be aligned with pursuit of healthful life.
Incentives in the form of modest co-pays, and the like, insulate consumers from the cost of health care. Consumers, rationally, are less price sensitive as a result. Consumers need to have incentive to be concerned about the cost of health services. Increasing price sensitivity of consumers will increase pricing pressure on health care providers.
3. Empower innovation. Innovation is the only path to reducing the cost of health services while simultaneously increasing the quality of health care. Encourage entrepreneurs to do what they do so well: create effective solutions to problems. Innovation is needed in myriad areas, including diagnostic and delivery technologies and in business models. Christensen, in The Innovator's Prescription: A Disruptive Solution for Health Care
A challenge of innovation is that innovation spurs changes in consumer expectations. Expectations re. what the health care system can deliver (e.g., ., what can be treated) are a function of the system's ability to innovate and get rewarded for that innovation. The more the system can deliver, the more we expect of the system; the more treatment we expect to be included in our health care coverage.
4. Focus on outcomes rather than inputs or specific solutions. A focus on outcomes spurs innovation that can yield better outcomes at lower costs. A focus on outcomes is consumer-centric; it puts the focus on quality of patient care rather than on the caregiver.
5. Health care, is a complex adaptive system. System improvement is a function of the system being able to cycle, adapt, and 'emerge'. This implies identifying and removing barriers that inhibit system innovation and adaptation.
6. The market is smarter than any individual entity (human or organization). Ergo, the health care system will operate most efficiently -- yielding the optimal patient outcomes -- when barriers to market function are systematically identified and removed.
These thoughts are necessarily incomplete and preliminary.

Cash for Clunker (in)Competence

Hundreds of auto dealers in the New York area have withdrawn from the government's Cash for Clunkers program, citing delays in getting reimbursed by the government, a dealership group said Wednesday.
The Greater New York Automobile Dealers Association, which represents dealerships in the New York metro area, said about half its 425 members have left the program because they cannot afford to offer more rebates. They're also worried about getting repaid.And Obama expects us to believe claims that expanding government involvement in the health sector will improve quality of care and reduce costs?
Sunday, August 16, 2009
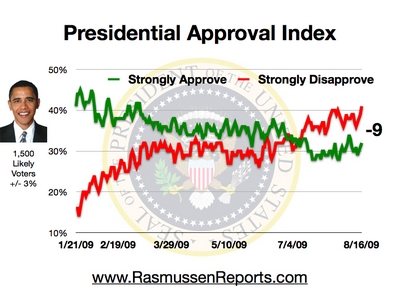
Obama's Negatives Continue to Build
Obama scores a -9 in Rasumssen's latest Presidential approval tracking poll:

That the strongly disapproves and strongly approves both ticked up in this latest poll may suggest that the middle is tipping toward strongly disapprove. The data also suggest public opinion is trending against Obama.. This tweaking of Rasmussen's graph emphasizes Obama's reversal of fortune:

That the strongly disapproves and strongly approves both ticked up in this latest poll may suggest that the middle is tipping toward strongly disapprove. The data also suggest public opinion is trending against Obama.. This tweaking of Rasmussen's graph emphasizes Obama's reversal of fortune:

Apple is Enablng 2009 to be 1984
Apple's famous '1984' ad concluded, "On January 24th, Apple Computer will introduce MacIntosh. You'll see why 1984 won't be like "1984":
Scott Ott illustrates how Apple is enabling 2009 to be like "1984". Yep, there's an app for that:
Scott Ott illustrates how Apple is enabling 2009 to be like "1984". Yep, there's an app for that:
The Health Care Diversion: It's the Economy, Stupid

One has to wonder: Is the Democrat's emphasis on health care a diversionary tactic? Sure, there is room for improvement in the U.S. health care system. Is a whole-sale make-over of the U.S. health care system needed? I don't read the tea leaves that way.
The momentum for whole-sale reform of the U.S.'s health care system is premised on a sour U.S. and world economy. The logic may go thus: The more people there are out of work, the more people there are that may be interested in government health care. Hence, the Obama administration has incentive to delay the recovery of the U.S. economy to increase the likelihood of passing government-run health care. My intent here is not to be conspiratorial. However, Rahm Emmanual's infamous, "Don't waste a 'serious crisis" comment, affords a basis for skepticism. The depressed U.S. economy affords just such a 'crisis' that can be 'leveraged.'
Issues with the U.S. health care system are meaningfully a function of the state of the U.S. economy. The healthier the U.S. economy, the more wealth there is available in the private sector. Wealth in the private sector reflects job creation, salary and benefits expansion, increased charitable giving to non-profit hospitals and other community support organizations, and greater freedom of individual choice. These, collectively, reduce the need for government involvement in health care.
The current government efforts to reconfigure the U.S. health care system reflect an attempt to address perceived systemic symptoms without an initial diagnosis. Proposed measures are akin to treating a fever generated by a bacterial infection with an ice-pack. The ice-pack is noticeable, and appears to offer relief, yet has no therapeutic impact on the underlying infection.
The considerable effort pouring into health sector reconfiguration focuses on a symptom that diverts energy and attention away from the underlying weakness of the U.S. economy. The focus on health sector reform is a diversion that pulls energy and focus away from engaging discussion on what is needed to ensure the long-term health of the U.S. economy; to engage entrepreneurial efforts that create jobs; to divert attention away from the fact that the U.S. economy continues to shed jobs.
To reprise a phrase popular with the last Democrat to occupy the White House: It's the economy, stupid. Getting the U.S. economy back on solid footing would seem to go a long way to improving the health care experience of every U.S. citizen and do so in a way that generates, rather than consumes, wealth and health for all.
The IRS and Your Health Care

Under both the House and Senate Health, Education, Labor and Pensions (HELP) Committee bills released to the public, the Internal Revenue Service will play a key role in monitoring and enforcing health care mandates against individual taxpayers. Yet the introduction of the IRS into the health care system has received scant attention.
The Senate bill imposes a new requirement that all persons who provide health care coverage to others must file a return with the IRS listing the names, addresses, social security numbers, and the coverage period for each person, and "such other information as the Secretary [of Health and Human Services] may prescribe." (Section 161(b) starting at page 107). The bill does not limit what information the Secretary may request, so it is conceivable and likely that information as to the nature of the coverage, the family members included, and other details will be reported to the IRS.
Read the whole thing. Would you want the IRS to be monitoring your health care and have the power to decide whether you have paid properly for care received?
Subscribe to:
Posts (Atom)